



What a Specialised Knee Pain Rehab Trainer can do for you.
No one likes sitting in the side-lines, but if we’re suffering from knee pain it can feel like there is no other way to go.
The knee is the longest and most complex joint in our body.1,2
Made up by several bones, muscles, ligaments and tendons, and surrounded by bursae and other tissues, the knee is designed to provide stability and movement.2
Because of its complexity, it is also very susceptible to injury; especially in any kind of contact sport.
Knee injuries are extremely common in people of all ages and backgrounds.3
With a plethora of causes ranging from trauma to overuse, living with knee pain can be exhausting and debilitating.
Among the most common injuries are sprains, especially in the ACL, meniscal tears, patellofemoral pain and osteoarthrosis caused by overuse.
Pain is our body’s way of saying that something is not working properly and should never be ignored.
If you live in London and have suffered an injury or are experiencing knee pain, a visit to a Knee Injury Rehabilitation Specialist can set you free.
From decreasing your pain to regaining strength and returning to play, a thorough evaluation and the right combination of exercises can get you back to living life to its fullest in no time.

Visiting a Knee Specialist
Knee pain can seem harmless and, in many cases, years can go by without it becoming significant enough to impair our day to day activities.
Nonetheless, an injury or ailment of the knee can gradually lead to compensatory postural and gait changes
that will in turn lead to a more severe disability.4
Injuries to the knee are extremely common in people of all ages and backgrounds.1 In itself, knee pain is simply a symptom to one of many underlying causes.5
Ranging from trauma, such as a football player being tackled on the field, to overuse, each one requires a specific course of action and associates with unique rehabilitation goals.
Chronic medical conditions such as obesity, gout, diabetes and autoimmune disorders like rheumatoid arthritis are a common source of knee pain.
When a person is overweight, their whole bodies are put to the test.
As the weight increases, the body is less and less likely to resist the loads it is submitted to.
As a matter of fact, for every extra kilogram of weight you add, your knees gain 4 kilograms of extra pressure in each step.6
Obesity is the single most important factor in the development of severe knee osteoarthrosis.6,7,8
Other chronic illnesses associated with knee pain include gout, a type of inflammatory arthritis, which is caused by high concentrations of uric acid.9
The excess uric acid begins to form crystals in different joints that lead to sudden bouts pain, swelling and tenderness.
In more severe cases, there is a limitation in the range of motion of the knee which can cause instability and dysfunction in the Anterior and Posterior Cruciate ligaments.9
In the autoimmune spectrum, rheumatoid arthritis, which affects mainly women, is often a cause of join pain and swelling.10
Unlike chronic medical conditions which develop through time, a traumatic injury to the knee can happen at any point of our lives and due to multiple circumstances.
From a car accident to getting tackled in a football match, a hit to the knee can cause pain, swelling and inflammation.
Depending on the severity of the injury and the tissues compromised, the knee rehabilitation process could require surgery and, according to the specific prognosis, several weeks or months of intense guided sessions.
Female athletes have a higher risk of developing knee pain and injury because of their anatomy.11
Wider hips enable women to carry a baby to term during pregnancy and undergo labour.
However, it also increases their Q Angle measured between the middle of patella (knee bone) and the Anterior Superior Iliac Spine (bony prominence in the pelvis).12
This angle has been associated with a lateral deviation from the regular path the patella follows during movement.
On average, women have up to 4.6º more than men in their Q Angle.
The larger is it, the higher the chances of lateral patellar tracking; associated with pain, swelling and chondromalacia (a deterioration of the cartilage on the inside surface of the patella).13
We have been led to believe that as we age, joint pain is a common occurrence.
In reality, no pain is our body’s protective mechanism indicating that something is not right.
Overuse injuries are quite common and often go untreated.
They occur when the body is subjected to constant stimulus without proper rest (such as rigorous training every single day) or when the stimulus is too strong for the body to handle (a sudden increase in load for an exercise).
If I have never gone out for a run and sign up for a 5-kilometre race without training, I will be subjecting my joints to a sudden and unexpected stimulus and they likely will react violently and negatively.
Visit a Knee Specialist today! Contact us for a FREE CONSULTATION If you have any questions or concerns, please contact Jazz Alessi, our knee rehabilitation specialist, at: 020 3633 2299 (Monday – Fri: 6:30am to 9pm – Saturday: 8am to 3pm).
For more information on knee conditions, procedures, rehabilitation and services offered at our website, please visit https://www.personaltrainingmaster.co.uk
Knee Injuries: Stressful, Costly and Emotionally Draining.
Getting injured can be a stressful, costly and emotionally draining process.
Whether traumatic by nature or developing through time, a knee injury can be very frustrating.
As mentioned previously, the knee is the largest and most complex joint in the body and for this reason is likely to need multiple studies to determine exactly what kind of injury you have suffered and what can be done to fix it.1
No two injuries are ever the same which means that even when the mechanism of injury might be similar, the tissues affected, the extent of the injury and its prognosis can greatly vary.14
If the injury is traumatic, such as would happen in a motor vehicle accident, it is likely that doctors will ask for scans and diagnostic imaging to determine the degree of injury.
Nonetheless, as the natural reaction from our body to injury is inflammation, initial scans and images might not be enough to determine accurately the prognosis and course of action to follow.
For this reason, physicians are likely to do a follow-up examination a few days after the injury (especially if it is limited to internal tissues such as ligaments and meniscus) to allow the swelling to decrease and obtain a clearer image of the damage.
More serious traumatic injuries such as exposed fractures will more than likely require immediate surgery as they can be life threatening.15
Once surgery has been performed, the physician will provide an outline for the course of rehabilitation including what to do and what to avoid.
A physiotherapist or a knee rehabilitation specialist should be the next professional to visit if you haven’t done so already.
Rehabilitation is a process that requires in-depth evaluation to determine not only the limitations in function, activity and participation associated to the injury but also other contextual factors that might affect each person’s individual recovery period.
Two people that suffered an ACL injury might have different rehabilitation expectations as one is a 20-year-old athlete wishing to return to play and the other is a 65-year-old retired man who occasionally exercises.
Don’t let knee pain get you down! Contact us for a FREE CONSULTATION. If you have any questions or concerns about our Knee Rehabilitation programme, please contact Jazz Alessi at: 020 3633 2299 (Monday – Fri: 6:30am to 9pm – Saturday: 8am to 3pm).
Knee Injury and Pain: Rehabilitation in London
Is pain always due to injury?
Knee pain does not always imply injury.
Mild inflammation of tissues in the knee due to strenuous activity, an unusual movement or even something as simple as wearing new shoes can certainly cause pain but it does not necessarily mean that the tissues are injured.
In these cases, rest and ice are recommended to alleviate acute pain which should subside fairly quickly.15
If the pain is persistent for over a week or seems to worsen as days go by, a visit to a knee rehabilitation specialist can provide some insights into the cause and best course to follow.
Constant or Sporadic Knee Pain?
As mentioned before, knee pain is never normal but the frequency of its appearance can provide some valuable information as to what might be causing it.
If you have not experienced any kind of trauma or hit to the knee and have sudden, sharp knee pain it could be associated to an underlying condition such as gout.
In contrast, if the symptom occurs only when performing an exercise or after exercising, it could be associated to poor posture, incorrect footwear or a load much too strenuous for the body to tolerate.
Pain that is constant and does not subside could be related to osteoarthrosis or degeneration of the cartilage in the knee joint.15
Is surgery always the best way?
Surgery is not the only rehabilitation mechanism but it can certainly prove to be the best in some cases.
While there are plenty of injuries that can be treated with physiotherapy and the correct personal training rehabilitation protocol, more severe injuries in which tissues have sprained or ruptured may have better outcomes when undergoing surgery.
An example is a complex ACL (Anterior Cruciate Ligament) injury that also affects the MCL (Medial Collateral Ligament).
If this injury occurs in a young athlete, the possibilities of return to play are much better with surgery and the appropriate rehabilitation process that follows.16
When should I start my rehabilitation process?
Sooner is better when it comes to rehabilitation.
Pre-operative therapy is one of the most important pieces to a successful recovery.
Although certain adaptation might be needed not to jeopardise or further damage the injured tissues, the rest of the body must prepare for a higher demand during the pre and post-surgical period.
Strengthening and conditioning your other leg and your arms will play a huge role in early mobilization after surgery and the overall results of the rehabilitation process.

Unsure if your knee pain is associated to a more serious injury? Contact us for a FREE CONSULTATION from our knee rehabilitation specialist. If you have any questions or concerns, please contact Jazz Alessi at: 020 3633 2299 (Monday – Fri: 6:30am to 9pm – Saturday: 8am to 3pm).
Knee Injury Risks
Injuries are unpredictable.
Even with proper technique when exercising, appropriate rest periods and training routines and a healthy lifestyle, an injury can happen when we least expect it.
Nonetheless, there are many risk-factors associated to knee injuries that can be prevented.
ACL (or Anterior Cruciate Ligament)
The ACL is one of the most commonly injured structures in the knee; especially in female athletes.
About 70 % of ACL injuries in athletes happen through mechanisms such as pivoting, cutting, sidestepping, out of control play or awkward landings, while about 30 occur from contact with other players.
A sprain happens when the ligament is overextended while a tear happens when it is stretched past its maximum extensibility.
In many cases, ACL injuries are accompanied by MCL injuries.11
PCL (or Posterior Cruciate Ligament)
PCL injuries are less common than ACL ones.
Normally, PCL injuries occur from a direct hit to the shin bone, as would happen in a car accident, or a fall onto the leg with the foot pointing down.
Unlike ACL injuries, isolated PCL injuries do not present a feeling instability.
For this reason, a non-surgical approach which includes physiotherapy and rehabilitation exercise is often recommended on isolated PCL tears.17
MCL (or Medial Collateral Ligament)
The MCL is located on the inside portion of the knee and provides stability to the inner knee restricting the knee from caving in.
The usual mechanism of trauma for MCL injuries is a hit to the outside of the knee that causes the knee to cave in suddenly.
Depending on how severe the hit is, injuries can range from a strain to a rupture.
In severe ACL injuries, the MCL can also be injured.11
LCL (or Lateral Collateral Ligament)
The LCL is located on the outside portion of the knee and provides stability to the outer knee restricting the knee from caving out.
These are the least common ligament injuries because the mechanism of trauma involves a hit to the inside of the knee that causes it to cave outwards.
Although less common, they are usually more debilitating than MCL injuries.18
Meniscus tears
Tearing of the meniscus occurs from forceful twisting of the knee while planted on the ground (bearing weight).
Also, it can occur during squatting or hyperflexion of the knee, after jumping and landing with a flexed knee or from twisting as the foot hits an obstacle (like a hole, rock or uneven surface).
The most common symptoms experienced include a popping sound when twisting followed by swelling and a “locked knee” that is hard to straighten
If the rupture is large enough a piece of torn meniscus can get trapped between the femur and tibia making it impossible for the knee to extend and requiring surgery to “unlock” it.19
Meniscus tears can have long term effects on the health of the knee joint.
Since the menisci are designed to bear weight and cushion to prevent bone to bone contact, its erosion can lead to the development of osteoarthritis.
Patellar Maltracking (Patellar Ligament)
Patellofemoral pain syndrome is a very common problem in adolescents and active young adults.
It occurs when nerves sense pain in the soft tissues such as tendons, the fat pad beneath the patella and bone around the kneecap.20
Similarly, it can be caused when the patella moves through the grove between the condyles.
When the knee is bent, the patella is pushed out to one side of the groove which may cause increased pressure between the back of the patella and the femur, irritating soft tissues.20
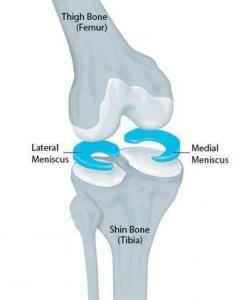
Meniscus Physical Therapy and Rehabilitation in London
Knee Meniscus Tear Recovery can be different depending on the area that was injured.
In the knee, there are fibrous cartilaginous structures in the top of the tibia called menisci.
Each knee has two menisci:
- a medial meniscus located on the inside part and a
- lateral meniscus located on the outside.
These structures are important primary stabilisers and weight transmitters of the knee; acting as shock absorbers that redistribute contact forces to the tibiofemoral joint and reducing friction within the joint.19,20,21
As mentioned previously, tearing of the meniscus can occur from forceful twisting of the knee while planted on the ground – bearing weight, squatting or hyperflexion of the knee, after jumping and landing with a flexed knee or from twisting as the foot hits an obstacle .19,20
Surgery is not always needed to repair the Meniscus.
The outer third of the meniscus (often called the red zone) is rich in blood and is likely to repair itself with time.
The two inner thirds (called the white zone), however, do not have blood supply making them unable to repair themselves and requiring surgery.
In these cases, an arthroscopy is the surgical method of choice.
The torn meniscus can then be trimmed or sutures can be placed to repair the damage.21
If surgery is not needed, an initial rehabilitation protocol of rest, ice, compression and elevation (RICE) is used to alleviate the pain and swelling.
Taking a break from physical activity is probably a good idea for the first few days and avoid bearing weight on the injured leg.
Initial rehabilitation protocol starts by restoring the range of motion of the knee and being able to extend and flex the knee with little to no pain.
Stretches will also be important to try to preserve the flexibility and extensibility of muscles surrounding the injured area.
When weight bearing is possible, exercises such as toe raises and straight leg raises will allow you to slowly gain strength.21
We can divide the recovery process into three separate stages.
During initial stages, physicians usually recommend the use of crutches to avoid weight bearing on the recovering leg.
For this stage it is essential to learn the appropriate way to use the crutches to avoid postural and overuse injuries to the other leg, arms and body.
Starting with isometric exercises, those in which the muscle is activated without having to move, your routine will target strengthening key muscles like:
- the quadriceps,
- hamstrings and
- glutes.
Isometric quadriceps exercises (like pressing down on rolled up towel under your thigh) or straight leg raises are key exercises in this stage.21

As the swelling starts to decrease and the tissues heal, you will start working on increasing the range of motion.
This process will get you to gradually leave the crutches behind and start working on weight bearing and walking normally again.
For this stage, your routine will continue to focus on building strength and knee stability but prioritise gaining a full range of flexion and extension.
A stationary bicycle is a fabulous tool during this stage as it starts to work on both flexion and extension of the knee as well as strengthening
Swimming and pool exercises are also helpful as it allows you to work on weight bearing and walking normally progressively. 20
During the final stage of recovery, the person is ready to return to normal daily life.
This stage focuses on continuation of the strength and conditioning routines for the whole body to prevent a relapse or a similar injury in the future.
If you are an athlete, this is the stage where you start to focus on return to play and specific sports-oriented training. 19, 20
Start your Meniscus Recovery Programme with the best! Book an appointment session with elite personal trainer in London.
Seven Steps to Rehab the Right Way
There are seven simple steps that you can follow to maximise the rehabilitation process of knee injuries.
Like in any recovery process, an injury will have stages of recovery in which certain movements or actions might be ideal and others might be counter indicated.
Therefore, the following steps serve as a general guideline for most knee injury rehabilitation processes but must be reviewed with a physician or rehabilitation specialist to ensure they are adequate for you.
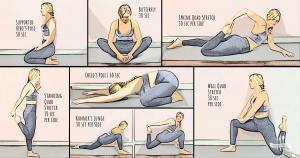
- Stretching to Improve Range of Motion
Stretching is an essential part of every exercise routine but often times the one that most people leave behind.
Muscles and tissues need to be warmed up before exercising and stretching provides the perfect opportunity to do so.
Dynamic stretching should be preferred over static when preparing to exercise.
Static stretching should be left for after exercising to relax the muscles used as it has been shown that using it before exercising can decrease performance due to fibre fatigue.23
- Improve Joint Strength
Strength is a crucial part of keeping the knee safe.
Good knee stability is one of the best ways to protect your knee from injuries and one of the first things that need to be regained after an injury.
Ligaments are the primary stabilisers of the knee, but they often fall short when preventing an injury.
Quadriceps strength exercises are one of the main focus of most ACL and knee injury recovery programmes – usually but, not always – the most affected.24
- Create Knee Stability
Our bodies have certain joints that are designed for mobility and some that are designed for stability.
While our hips and ankles are meant to provide plenty of movement, our knees should be stable.
After a knee injury, especially if a ligament is sprained or torn, a general feeling of instability can appear.
The rehabilitation process should focus from its early stages in rebuilding knee stability through strengthening and proprioceptive exercises.
This will reduce the likeliness of re-injury.
Patients with untreated instabilities, such as an ACL injury, are more likely to end up having meniscal surgery and other cartilage damage because of the misalignment of the bones.25
- Shed Unnecessary Weight
As mentioned previously, weight plays an essential role in the development of osteoarthrosis as well as other chronic conditions associated with knee pain.
If you are overweight, exercising can prove difficult and painful, especially if there are other conditions present such as diabetes, heart and metabolic diseases.
A knee rehabilitation specialist can guide you through the most effective and safe weight to shed some weight while ensuring that no injuries happen during this process. 6,7
- Use Myofascial Release
Myofascial release techniques are a wonderful tool to re-establish the mobility and flexibility of or tissues.
The fascia is a strong, web-like connective tissue that provides structure and stability to our body.
Tools like massage balls and foam rollers can be used to mobilise the fascia and release any restrictions that might be causing movement limitations as well as relieve muscular pain and stiffness after exercising.26
- Movement Variability
The first time you try running 1.5 kilometres can feel painful and exhausting.
Your body is not used to this activity and is unsure how to breathe and adapt.
With time and practice, your body will eventually develop adaptations to running that distance and it will start to feel easier.
Your body has adapted to this exercise and will need something more demanding for the body to continue creating adaptations.
The idea behind training is to provide different stimulus to our muscles and joints in order to generate adaptations.
If the stimulus is always the same, the body will adapt and it will no longer require adaptations.
For this reason, when rehabilitating an injury multiple exercises must be used to provide different experiences for the body to adapt to.
- Different levels training
Strength and flexibility are only part of what needs to be trained after an injury.
Coordination, proprioception (our ability to know where our extremities are located in space without looking), speed and endurance are all important elements that are often lost or diminished due to injury.
Readapting to these will often take place in more advanced stages of the rehabilitation process once stability and correct muscle activation are occurring.
Add on to the Seven Steps to Rehab the Right Way with a FREE CONSULTATION from our knee specialist!
If you have any questions or concerns, please contact Jazz Alessi, our knee rehabilitation specialist, at: 020 3633 2299 (Monday – Fri: 6:30am to 9pm – Saturday: 8am to 3pm).
Advanced Knee Rehab Exercises, Do it the Right Way
Choosing the correct exercises based on the type of injury, prognosis and rehabilitation goals is extremely important, but it is just as important to perform the exercises correctly.
Your advanced knee rehabilitation protocol will likely include some these exercises, so let’s review the correct way to do them.
Squats with A Weight
A squat is a very simple yet extremely beneficial exercise.
If done properly, squats are excellent for full body training and knee strengthening.
During the initial stages of rehabilitation, you will begin with bodyweight squats and progress to adding weight or other variations.
To adequately perform a squad, separate both legs to shoulder width and slowly descend as if you were trying to sit in an imaginary chair behind you.
The movement should be coming from your hips in a hinge motion with your knees bending as you descend.
During this process, your knees will go beyond the tip of your toes.
This is ideal and needed in order to fully obtain the range of motion needed.
When holding the weight, make sure you place it near your chest; avoiding a curved back when you descend.27
Bridging: Stage 2
The bridge is another common exercise used in rehabilitation protocols after knee injuries.
The initial steps of the rehab process will focus on teaching you the appropriate bracing techniques in order to maintain the correct posture throughout this exercise.
Once you understand how to brace the core and you can maintain a basic bridge position you can transition into more advanced variations.
The basic bridge involves laying down face up with your legs extended and our arms to the side. From this position, bend your legs and plant your feet at shoulder width.
This is your starting position.
Separate your glutes and back from the floor by first bracing your core and lifting.
Remember to keep the glutes activated through this exercise.
A more advanced version includes a straight leg hold bridge where you elevate one extended leg while holding the bridge position.28
Forward and Reverse Lunges
Lunges are great strengthening exercises for the thighs, glutes and calves.
There are a few variations for the lunge including a forward lunch where you step forward and a reverse lunge where you step back.
Although they target the same muscles, reverse lunges often prove safer as they provided less stress on the knees.
To properly execute a reverse lunge, start standing with your feet together and arms to your sides.
Lift your foot off and take a step back bending your forward knee to a 90º angle and lowering the back knee close to the floor.
To perform a forward lunge, follow the same steps as the reverse lunge but instead of the step back, take a step forward.29
Conclusion
The knee is the largest and most complex synovial joint in the body.
With two menisci, two main tendons, three bones and four ligaments, the knee is a perplexing hinge joint.
Build for stability and not mobility, the knee allows us to jump, swim, walk and sit.
Because of its complexity, it is oftentimes a site of injury; leading to surgery and extended rehabilitation processes.
Pain is our body’s way of saying that something is wrong.
Knee pain is a very common symptom in people of all ages and backgrounds.
Although pain is not always associated to a serious injury, it should not be considered normal.
Injuries to the can be caused by trauma, associated to other diseases or linked to overuse.
Although it can seem harmless and, in many cases, years can go by without it becoming significant enough to impair our day to day activities, no one should be living with pain.
Sports injuries are unpredictable and can happen in all ages and level of play.
The most common injuries are to the ligaments, especially the ACL and MCL and the Meniscus.
For ligament injuries, especially if there is tearing, surgery is often the recommended course of treatment followed by extensive physical therapy or rehabilitation services.
For meniscus injuries, depending on the area injured it can be treated with a simple rehabilitation protocol or with arthroscopic surgery.
Visiting a knee rehabilitation specialist is ideal when struggling with knee pain or injury.
A thorough evaluation and a progressively more challenging rehabilitation routine can make a big difference in the recovery of movement and strength needed for daily activities and, in the case of athletes, return to play.
Routines for recovery vary according to injury type and objectives.
The focus, however, will be the same for all injuries: to regain the abilities lost and to live a pain free life.
Contact us for a FREE CONSULTATION.
If you have any questions or concerns about our London 12 weeks Body Transformation program, please contact jazz Alessi at: 020 3633 2299 (Monday – Fri: 6:30am to 9pm – Saturday: 8am to 3pm).
Request for free consultation here https://www.personaltrainingmaster.co.uk/contactme/
For more information on conditions, procedures, and rehabilitation services offered at our website, please visit https://www.personaltrainingmaster.co.uk
Sources:
- Santos Salas, X. Non-traumatic knee pathology in adults: A pictorial review. https://doi.org/10.1594/ECR2018/C-3069
- Schoen, D.C., Adult Orthopaedic Nursing. Chapter 10: The Knee and the Lower Leg. Lippincott, Philadelphia, Pa.
- Strudwick, K., McPhee, M., Bell, A., Martin-Khan, M., Russell, T. Review article: Best practice management of common knee injuries in the emergency department (part 3 of the musculoskeletal injuries rapid review series). Emergency Medicine Australasia. https://doi.org/10.1111/1742-6723.12870
- Pietrosimone, B., Blackburn, J.T., Padua, D.A., Pfeiffer, S.J., Davis, H.C., Luc-Harkey, B.A., Harkey, M.S., Stanley Pietrosimone, L., Frank, B.S., Creighton, R.A., Kamath, G.M., Spang, J.T. Walking gait asymmetries 6 months following anterior cruciate ligament reconstruction predict 12-month patient-reported outcomes: GAIT AND OUTCOMES POST-ACLR. https://doi.org/10.1002/jor.24056
- Boudreau, S.A., Royo, A.C., Matthews, M., Graven-Nielsen, T., Kamavuako, E.N., Slabaugh, G., Thorborg, K., Vicenzino, B., Rathleff, M.S. Distinct patterns of variation in the distribution of knee pain. https://doi.org/10.1038/s41598-018-34950-2
- Atukorala, I., Makovey, J., Lawler, L., Messier, S.P., Bennell, K., Hunter, D.J. Is There a Dose-Response Relationship Between Weight Loss and Symptom Improvement in Persons With Knee Osteoarthritis? Weight Loss and Symptomatic Knee OA Improvement. Arthritis Care & Research. https://doi.org/10.1002/acr.22805
- Christensen, R., Bolvig, J., Lund, H., Bartels, E.M., Astrup, A.V., Hochberg, M.C., Singh, J.A., Lohmander, S., Bliddal, H., Juhl, C.B. Weight loss for overweight patients with knee or hip osteoarthritis. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD012526
- Li, J.-S., Tsai, T.-Y., Clancy, M.M., Li, G., Lewis, C.L., Felson, D.T. Weight loss changed gait kinematics in individuals with obesity and knee pain. Gait & Posture. https://doi.org/10.1016/j.gaitpost.2018.12.031
- Jabalameli, M., Bagherifard, A., Hadi, H., Behshad, V., Ghaffari, S. Chronic tophaceous gout. https://doi.org/10.1093/qjmed/hcx019
- Arendt-Nielsen, L. Pain sensitisation in osteoarthritis. Clin. Exp. Rheumatol.
- Montalvo, A.M., Schneider, D.K., Yut, L., Webster, K.E., Beynnon, B., Kocher, M.S., Myer, G.D. “What’s my risk of sustaining an ACL injury while playing sports?” A systematic review with meta-analysis. https://doi.org/10.1136/bjsports-2016-096274
- Vora, M., Curry, E., Chipman, A., Matzkin, E. Patellofemoral pain syndrome in female athletes: A review of diagnoses, etiology and treatment options. https://doi.org/10.4081/or.2017.7281
- Almeida, G.P.L., Ana Paula de Moura Campos Carvalho e Silva, França, F.J.R., Magalhães, M.O., Burke, T.N., Marques, A.P. Q-angle in patellofemoral pain: relationship with dynamic knee valgus, hip abductor torque, pain and function. Revista Brasileira de Ortopedia https://doi.org/10.1016/j.rboe.2016.01.010
- Patel, D.R., Villalobos, A. Evaluation and management of knee pain in young athletes: overuse injuries of the knee. https://doi.org/10.21037/tp.2017.04.05
- Casey, E., Rho, M., Press, J.M. Sex differences in sports medicine.
- Siemieniuk, R.A.C., Harris, I.A., Agoritsas, T., Poolman, R.W., Brignardello-Petersen, R., Van de Velde, S., Buchbinder, R., Englund, M., Lytvyn, L., Quinlan, C., Helsingen, L., Knutsen, G., Olsen, N.R., Macdonald, H., Hailey, L., Wilson, H.M., Lydiatt, A., Kristiansen, A. Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline. https://doi.org/10.1136/bmj.j1982
- Resnik, A.M., Resnik, J.Y. A knee and shoulder handbook: for all of us. New Haven, CT.
- Cameron, P., Little, M., Mitra, B., Deasy, C., 2019. Textbook of Adult Emergency Medicine E-Book.
- van de Graaf, V.A., Noorduyn, J.C.A., Willigenburg, N.W., Butter, I.K., de Gast, A., Mol, B.W., Saris, D.B.F., Twisk, J.W.R., Poolman, R.W., Effect of Early Surgery vs Physical Therapy on Knee Function Among Patients with Nonobstructive Meniscal Tears: The ESCAPE Randomized Clinical Trial. https://doi.org/10.1001/jama.2018.13308
- Chevidikunnan, M.F., Al Saif, A., Gaowgzeh, R.A., Mamdouh, K.A. Effectiveness of core muscle strengthening for improving pain and dynamic balance among female patients with patellofemoral pain syndrome. https://doi.org/10.1589/jpts.28.1518
- Resnik, A.M., Resnik, J.Y. A knee and shoulder handbook: for all of us. New Haven, CT.
- Frizziero, A., Ferrari, R., Giannotti, E., Ferroni, C., Poli, P., Masiero, S., 2012. The meniscus tear. State of the art of rehabilitation protocols related to surgical procedures.
- Behm, D.G. The science and physiology of flexibility and stretching: implications and applications in sport performance and health.
- Dedinsky, R., Baker, L., Imbus, S., Bowman, M., Murray, L. Exercises that facilitate optimal hamstring and quadriceps co-activation to help decrease ACL injury risk in healthy females: a systematic review of the literature.
- Sheean, A.J., Shin, J., Patel, N.K., Lian, J., Guenther, D., Musahl, V. The Anterolateral Ligament is Not the Whole Story: Reconsidering the Form and Function of the Anterolateral Knee and its Contribution to Rotatory Knee Instability. https://doi.org/10.1097/BTO.0000000000000303
- Ferguson, L.W., Gerwin, R., Clinical mastery in the treatment of myofascial pain. Lippincott Williams & Wilkins, Philadelphia.
- Horschig, A., Sonthana, K., Neff, T., 2017. The squat bible: the ultimate guide to mastering the squat and finding your true strength.
- Contreras, B., 2019. Glute lab. Tuttle Publishing.
- Lee, D.G., 2011. The Pelvic Girdle: an Approach to the Examination and Treatment of the Lumbopelvic-Hip Region. Elsevier Health Sciences UK, London.