



So, you survived the first heart attack. A big caution here – you are at an increased risk of another one. In the UK, once every three minutes a patient goes to hospital due to a heart attack. Nearly one million people alive in the UK today have survived a heart attack [1].
It is important to realise that heart attack survivors are at the highest risk to develop future heart attacks especially shortly after the first attack.
Their annual death rate is five per cent, which is six times that for healthy people of the same age [2].
This is the case today despite the use of contemporary treatment options and modern technologies in therapy.
A repeat heart attack carries a significant risk of death or progression of coronary heart disease following the first heart attack [3].
An important scientific study has demonstrated that the risk for a repeat heart attack was highest in the first month with the risk markedly declining over the first 3 months.
However, it also showed that a repeat heart attack is particularly hazardous with a very high risk of death within ten days of 20.5 per cent [4].
The same study showed that patients who survive a repeat heart attack continue to be at very high risk for death (twice that of a single heart attack patient).
It also demonstrated that the rate of death at one year for those who had a repeat heart attack was 38.3 per cent (nearly four times that of a single heart attack patient) [4].
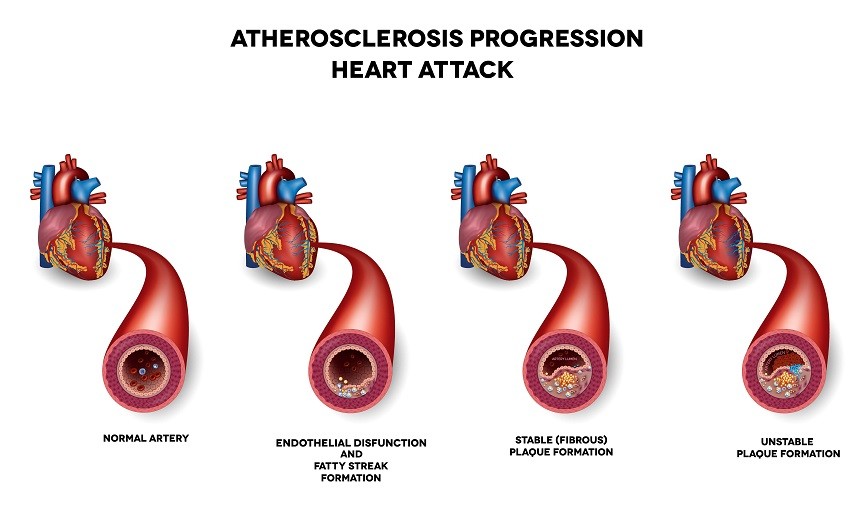
Scientific research has shown that experiencing a heart attack seems to speed up the process of atherosclerosis (deposition of fat inside the arteries).
This seems to be caused by the heart attack acting as a trigger that leads to the activation of certain processes inside the body which produce harmful chemicals (called inflammatory markers) that accelerate the progression of atherosclerosis and thus increase the likelihood of experiencing a repeat heart attack [5].
Risk Factors
The risk factors that could lead to the development of a repeat heart attack are quite like those that caused it in the first place, these are:
1. Continued smoking:
Following a heart attack, complete abstinence from smoking is reported to be in a range from 16 to 40 per cent. Continued smoking means continued risk [6].
2. High blood pressure:
Uncontrolled blood pressure causes injury to the coronary arteries and could cause a repeat heart attack. [7,8]
3. High blood sugar:
This accelerates the process of atherosclerosis by several mechanisms [7,8].
4. High blood cholesterol:
Especially the so called low-density lipoprotein cholesterol (harmful LDL-C) which causes fat deposition in the coronary arteries that may occlude implanted stents or coronary artery bypass grafts [7,8].
5. Age and gender:
Being over 65 years old and/or male is associated with an increased risk of repeated episodes [7,8].
6. Inactive lifestyle:
Lack of physical activity or regular exercise has negative effects on heart attack survivors [7,8].
7. Obesity and overweight:
A body mass index (a reflection of weight in relation to height) that is above 25 kg/m2 is associated with adverse outcomes [7,8].

8. Continued stress:
Lack of proper stress management, continued fears and anxiety, depression and having a negative stance towards social engagement all contribute to the development of a repeat heart attack [7,8].
9. Lack of medical follow up and non-adherence to medications:
Current medications significantly reduce the risk of repeat heart attacks and may even reverse the process of atherosclerosis [7,8]. That’s why prescribed medications should be rigorously followed.
10. Heart failure:
If the first heart attack resulted in reduction of the heart’s contractile (pumping) function, then the risk of developing a repeat attack is even higher due to associated heart failure [7,8].
11. Peripheral arterial disease (diseased arteries of the legs):
A person suffering from claudication pains (severe leg cramps during walking) caused by narrowing of the arteries of the legs usually has advanced coronary heart disease [9].
12. Kidney disease:
Reduced kidney functions are a strong risk factor for developing a repeat heart attack [10].
Some lifestyle changes can help prevent a repeat heart attack
Fortunately, there are several ways in which you can significantly reduce the risk of a repeat heart attack.
Scientific evidence has shown that aggressive interventions aimed at reducing risk factors after a heart attack help reduce the overall rates of death by decreasing the risk of a repeat heart attack [2].
It is important to strictly adhere to doctor recommendations, attend regular check-up consultations and receive all prescribed medications as instructed [8].

However, medications are only one of the four cornerstones of your therapy. The other three being lifestyle, eating habits and physical activity.
1. Lifestyle adjustments [8]:
This includes several interventions such as:
- Quitting smoking and not just cutting down.
- Reducing alcohol consumption to recommended levels or quitting altogether.
- Learning how to properly manage anxiety and stressful situations.
- Being positive and outgoing and leading an active, engaging life.
2. Eating habits:
The National Institute for Health and Care Excellence (NICE) guidelines here in the UK recommended the heart healthy Mediterranean diet [11].
The Mediterranean diet consists of [12]:
- Eating plant-based foods.
- Using healthy fats such as olive oil and canola oil.
- Using herbs and spices instead of salt.
- Enjoying meals with family and friends.
- An option of drinking red wine in moderation.
- Getting plenty of exercise.
3. Physical activity [11]:
The NICE guidelines in the UK recommend at least 20 to 30 minutes of moderate physical activity to the point of slight breathlessness.
People who are not active are advised to increase their activity in a gradual, manner to increase their exercise capacity.

They should start at a comfortable level and gradually increase the duration and intensity of activity as they gain fitness.
The benefit of exercise will be enhanced by customised advice from a suitably qualified professional.
These goals and more can be achieved by joining the so-called “Cardiac Rehabilitation Programmes” which are recommended after recovering from a heart attack.
Join a Cardiac Rehabilitation Programme to Reduce Repeat, Recurrent Heart Attacks
Cardiac rehabilitation has been scientifically proven to reduce the risk of death from a heart attack [13].
While a cardiac rehabilitation programme doesn’t change your past, it can help improve your heart’s future by significantly reducing the risk of a repeat heart attack.
Cardiac rehabilitation programmes are comprehensive programmes that include:
1. Exercise counselling and training [14]:
Exercise training is the cornerstone of cardiac rehabilitation programmes due to its positive effects in the form of:
- Stopping or reversing atherosclerosis.
- Improving the general psychological condition of heart patients.
- Reducing the risk of blood clot formation (by decreasing the production of chemicals responsible for clot formation and increasing those responsible for clearing them out from the circulation).
- Reducing the risk of developing heart attacks.

2. Education for heart-healthy living:
Healthy behaviour changes and education are another key component of cardiac rehabilitation programmes.
Participants are given detailed information about their heart’s condition and lifestyle advice, including:
- The cause of heart attacks.
- The risk factors and how to manage them.
- Common heart disease misconceptions.
- The importance of medication.
- The importance of smoking cessation.
- What constitutes a healthy diet.
- How to improve mobilisation through graded physical activity and the place of exercise for patients with heart disease.
Education is enforced during all phases of the programme some of which sometimes start before hospital discharge [14,15].
3. Psychological counselling:
Professional psychological counselling and stress management are an integral part of cardiac rehabilitation programmes.
Several scientific studies have demonstrated improvements in depression, anxiety, and so-called hostility scores after cardiac rehabilitation [16].
The specific impact of including such psychological and social interventions was assessed in scientific studies by comparing comprehensive programmes to exercise-only programmes. It was shown that a greater reduction in psychological distress was achieved in comprehensive programmes [17].
The impact of the psychological counselling performed during cardiac rehabilitation programmes was also examined in a review of 13 scientific studies for heart failure patients showing an important improvement in the Minnesota Living with Heart Failure questionnaire which is a highly recognised measure for quality of life in heart failure patients [18].
4. Clinical follow-up:
These are encouraged and supported throughout the programme.
5. Medical treatment optimisation:
This is performed by your doctor as your health improves and needs change during participation in the programme.
6. Risk factor modification:
This is achieved using the different tools that cardiac rehabilitation programmes provide through education, exercise, dietary advice and medical therapies.
All about cardiac rehabilitation
What is cardiac rehabilitation?
Cardiac rehabilitation is defined by the World Health Organization (WHO) as all activities and interventions required to ensure the best possible physical, mental, and social conditions so that patients with cardiovascular disease may, by their own efforts, preserve or resume their proper place in society and lead an active life [20].
In other words, cardiac rehabilitation is a comprehensive programme that includes exercise, education, and behaviour modifications with the goal of helping patients recovering from heart disease restore and maintain optimal health on the one hand and reducing the risk of repeat heart problems on the other.
Who is cardiac rehabilitation for?
Once they are cleared by a doctor, the following sets of patients should join a cardiac rehabilitation programme [21]:
- Survivors of heart attacks who have been adequately treated and have no remaining symptoms of an active disease.
- Stable heart failure patients who are on optimal medical therapy.
- Patients who had a coronary artery bypass surgery.
- Patients who had stents implanted in their coronary vessels via a heart catheterisation procedure.
- Those who had a heart transplantation.
- Patients with stable coronary heart disease.
- Patients seen after valve surgeries.
Cardiac rehabilitation programmes
For a cardiac rehabilitation exercise programme to be successful it is necessary to have the following:
- A multidisciplinary approach:
A team effort is required to help you achieve your goals.
This requires close collaboration between your doctor, physical therapist/exercise trainer, and nutritionist.
In addition, a support network is provided for social and psychological reintegration.
- Commitment:
A strong will to commit to the whole length of the programme is mandatory as this is how benefits will be achieved.
According to scientific research, all benefits come from completing the whole programme and not just attending a few sessions.
That’s why it is required to complete the programme fully to benefit from the massive life-changing benefits that a cardiac rehabilitation programme has to offer.
- Customisation:
No patient should be denied a cardiac rehabilitation programme but not all patients are the same.
Hence the programme should be designed in a customised fashion for each patient based on the current medical condition and physical ability with specifically designed goals for each patient to achieve accordingly.
- Proper exercise training:
A properly designed and reliable cardiac rehabilitation exercise programme is the key element for success.
Exercise has been shown to be responsible for a major part of the benefits incurred by a cardiac rehabilitation programme.
Personalised Cardiac Rehabilitation Programmes by Jazz Alessi
I am an Elite Personal Trainer, Clinical Exercise Specialist, Second Generation Pilates Trainer, Certified Nutritionist and Weight Loss Expert.
I have worked closely with many patients suffering from heart disease and achieved stunning results.
I specifically tailor my programmes to your needs depending on several factors to help you achieve your goals.
I always aim at helping you get the quality of life you deserve through a personally designed programme that is both safe and effective.
References:
- British Heart Foundation. Cardiovascular Disease Statistics 2017.
- WHO. Prevention of Recurrences of Myocardial Infarction and Stroke Study: The PREMISE programme. 2017.
http://www.who.int/cardiovascular_diseases/priorities/secondary_prevention/country/en/index1.html
- Thune J, Signorovitch J, Kober L, et al. Predictors and prognostic impact of recurrent myocardial infarction in patients with left ventricular dysfunction, heart failure, or both following a first myocardial infarction. Eur J Heart Fail. 2011;13:148–153. doi: 10.1093/eurjhf/hfq194
http://onlinelibrary.wiley.com/doi/10.1093/eurjhf/hfq194/full
- Pfeffer MA, McMurray J, Leizorovicz A, et al. Valsartan in acute myocardial infarction trial (VALIANT): rationale and design. Am Heart J. 2000;140:727–750.
http://www.ahjonline.com/article/S0002-8703(00)09750-7/fulltext
- Wang H, Eitzman D. Acute myocardial infarction leads to acceleration of atherosclerosis. Atherosclerosis. 2013 Jul;229(1):18-22. doi: 10.1016/j.atherosclerosis.2013.04.004.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3691345/
- Grandi S, Eisenberg M, Joseph L, et al. Cessation treatment adherence and smoking abstinence in patients after acute myocardial infarction. Am Heart J. 2016 Mar;173:35-40. doi: 10.1016/j.ahj.2015.12.003.
- Thune J, Signorovitch J, Kober L, et al. Predictors and prognostic impact of recurrent myocardial infarction in patients with left ventricular dysfunction, heart failure, or both following a first myocardial infarction. Eur J Heart Fail. 2011 Feb;13(2):148-53. doi: 10.1093/eurjhf/hfq194.
http://onlinelibrary.wiley.com/doi/10.1093/eurjhf/hfq194/full
- Colantonio L, Bittner V. Managing residual risk after myocardial infarction among individuals with low cholesterol levels. Cardiol Clin. 2015 May;33(2):299-308. doi: 10.1016/j.ccl.2015.01.004.
- Inglis S, McMurray J, Böhm M, et al. Intermittent claudication as a predictor of outcome in patients with ischaemic systolic heart failure: analysis of the Controlled Rosuvastatin Multinational Trial in Heart Failure trial (CORONA). Eur J Heart Fail. 2010 Jul;12(7):698-705. doi: 10.1093/eurjhf/hfq070.
http://onlinelibrary.wiley.com/doi/10.1093/eurjhf/hfq070/full
- Anavekar N, McMurray J, Velazquez E. Relation between renal dysfunction and cardiovascular outcomes after myocardial infarction. N Engl J Med. 2004 Sep 23;351(13):1285-95.
http://www.nejm.org/doi/full/10.1056/NEJMoa041365
- National Institute for Health and Care Excellence. Secondary prevention in primary and secondary care for patients following a myocardial infarction. Clinical guideline 172. London: National Institute for Health and Care Excellence (NICE); 2013.
https://www.ncbi.nlm.nih.gov/pubmedhealth/n/nicecg172/pdf/
- Mayo Clinic. Mediterranean diet: A heart-healthy eating plan. 2017
- Oldridge et al. Cardiac Rehabilitation After Myocardial Infarction – Combined Experience of Randomized Clinical Trials. JAMA 1988;260:945-950. doi: 10.1001/jama.1988.03410070073031
https://jamanetwork.com/journals/jama/article-abstract/373499
- Dalal H, Doherty P, Taylor R. Cardiac rehabilitation. BMJ. 2015 Sep 29;351:h5000. doi: 10.1136/bmj.h5000.
http://www.bmj.com/content/351/bmj.h5000
- Bethell H, Lewin R, Dalal H Cardiac rehabilitation in the United Kingdom Heart 2009;95:271-275.
- Lavie C, Milani R. Adverse psychological and coronary risk profiles in young patients with coronary artery disease and benefits of formal cardiac rehabilitation. Arch Intern Med. 2006 Sep 25;166(17):1878-83.
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/410922
- Linden W, Stossel C, Maurice J. Psychosocial interventions for patients with coronary artery disease: a meta-analysis. Arch Intern Med. 1996 Apr 8;156(7):745-52.
https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/621809
- Sagar V, Davies E, Briscoe S, et al. Exercise-based rehabilitation for heart failure: systematic review and meta-analysis. Open Heart2015;2:e000163
- Bethell H, Lewin R, Dalal H. Cardiac rehabilitation in the United Kingdom. Heart2009;95:271-5
- WHO Expert Committee on Rehabilitation. World Health Organ Tech Rep Ser 1993;831:1122.
- Thomas et al. AACVPR/ACC/AHA 2007 performance measures on cardiac rehabilitation for referral to and delivery of cardiac rehabilitation/secondary prevention services. JACC 2007 Oct 2;50(14):1400-33. doi: 10.1016/j.jacc.2007.04.033.
Disclaimer: This website and all its content is to be used for information purposes only. This website or any of its content or links to third parties does not diagnose, advise, treat or cure any ailments, illness or disease.
You agree to hold harmless the owner of this site for any action taken on your own without consulting your medical doctor first by using the information on the website for diagnostic, treatment, or any other related purposes. This is not medical advice. If you are suffering from any illness, disease or ailments please contact your doctor first and immediately.