


Any form of sports activity is very complex, and requires the musculoskeletal system to be healthy and strong. Any sort of injury to the body, especially the musculoskeletal system disturbs the body mechanics, which if not taken care of can cause permanent damage.
Any over-stretching or tearing of your anterior cruciate ligament (ACL) in the knee can lead to an anterior cruciate ligament (ACL) injury. This tear can be partial or complete.
Knee Joint Overview
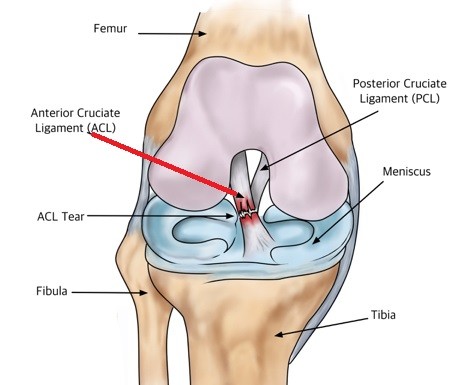
The knee joint is located where the end of the femur (thigh bone) fixes with the top of the tibia (shin bone).
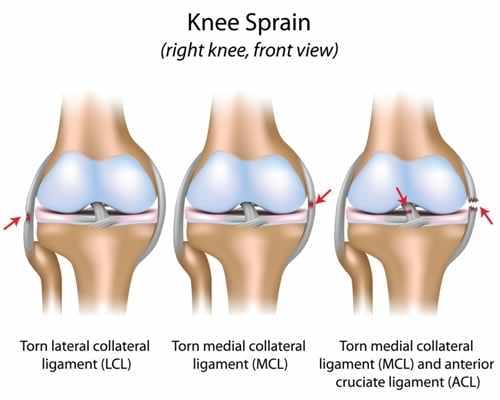
The knee has four main ligaments that connect the femur and tibia:
- Medial collateral ligament (MCL): The ligament runs along the inside of the knee. It prevents internal bending of the knee.
- Lateral collateral ligament (LCL): The ligament runs along the outside of the knee. It prevents external bending the knee.
- Anterior cruciate ligament (ACL): The ligament runs in the middle of the knee. It prevents the shin bone from sliding out in front of the femur.
- Posterior cruciate ligament (PCL) works with the ACL. It prevents the tibia from sliding backwards under the femur.
Do you have a knee injury question you’d like to be answered?
What can lead to injury to the ACL
You can have an ACL injury if you:
- Get hard hit on the side of your knee, such as during a football tackle
- Overextend your knee joint
- Stop moving suddenly or abruptly change direction while running or jumping
Basketball, football, soccer, and skiing are other common sports injuries, which can lead to ACL tear.
ACL tears are common in the middle of the ligament. These injuries form a gap between the torn edges, which do not heal on their own.
An alteration in the mechanisms of neuromuscular control can also increase the knee load and make it susceptible to ACL injury. In addition, the stability of trunk is associated with the distal body parts. Any defect in the neuromuscular control of the trunk may increase the abduction of the knee and adduction at the hip. This sudden twisting motion may lead to an ACL injury.
Warning signs that you have an ACL tear
During the initial phase of injury, you may hear a “popping” sound from the knee. There may be swelling around the knee within 6 hours of injury. You may have pain if you try doing any strenuous activity, like bearing weight on the affected knee, and the knee joint may undergo an abrupt instability.
Immediately visit your health care provider under such condition.

Avoid playing sports or other activities until you have been treated.
Your provider may send you for a knee MRI (Magnetic Resonance Imaging) to confirm the diagnosis. An MRI is the most preferred choice of detecting an ACL tear.
Would you like to get rid of your knee pain, and successfully rehabilitate your ACL injury?
Contact us now through this link, HERE.
After the MRI confirms the presence of an ACL tear, the initial treatment for an ACL injury may include:
- Rest the injured limb and avoid any movement
- Cryotherapy (applying ice on the knee)
- Compression of the knee with a compression bandage
- Raising your leg above the level of the heart
Other treatments may include:
- Pain relieving medicines, such as nonsteroidal anti-inflammatory drugs (ibuprofen)
- Crutches to walk until the swelling and pain get better
- Physical therapy to help improve joint motion and leg strength
- Surgery to rebuild the ACL
Treatment following an ACL reconstruction depends on your age, the level of activity and the influence of sports in your life. In case of chronic complete tears surgery is the only option. However, surgery is not the option for elderly patients as they do not tend to complain of knee instability with recreational activities.
ACL reconstruction or surgery for managing the ACL tear
ACL reconstruction is surgery to restructure the anterior cruciate ligament. As discussed earlier, the ACL holds your tibia in place.
The surgery
ACL surgery is usually performed with patients in lying in supine position. Most patients are given general anesthesia right before surgery. Other kinds of anesthesia, like regional anesthesia or a block, may also be used.
The tissue to restore your damaged ACL may either be taken from your own body or from a donor.
Tissue taken from your own body is called an autograft. The two most common sites preferred to take tissue from are the knee cap tendon or the hamstring tendon (Hamstring is the muscle behind your knee). On the other hand, tissue taken from a donor is called an allograft.
The procedure is usually performed with knee arthroscopy. During arthroscopy, a tiny camera is inserted into the knee through a small surgical cut. The camera is connected to a video monitor in the operating room. The surgeon uses the camera to check the ligaments and other tissues of knee.
The surgeon makes other small cuts around your knee and inserts other medical instruments to fix any other injury present. The surgeon then replaces the torn ACL by:
- Removing the damaged part of the torn ligament using a shaver or other similar instruments.
- Making a bigger incision to make room for the removal of autograft.
- Making tunnels in the bone to make space for the new tissue, which will take the place as the former ACL.
- Attaching the new ligament to the bone with screws or other devices to fix it in place. As healing progresses the tunnels in the bones fill in holding the new ligament in place.
At the end of the surgery, the surgeon closes the incisions with sutures and cover the area with a dressing.
Would you like to get rid of your knee pain, and successfully rehabilitate your ACL injury?
Contact us now through this link, HERE.
Rehabilitation following ACL repair
The aim of rehabilitation program following an ACL reconstruction is to gain full range of motion (ROM) and increase strength around the knee joint.

Over the last few years, there has been a progressive change observed in the rehabilitation of ACL.
Initially, immobilization was considered as the key to manage the knee instability following ACL reconstruction.
However, recent researches lay an emphasis on strength training for treating ACL tear.
Researches have said that the traditional practices of resistance training, cardiovascular exercise and agility drills do not play much role in managing the ROM around the knee.
The initial rehabilitation following an ACL repair mainly focuses on brace (either a knee immobilizer or a hinge brace) and Continuous Passive Motion (CPM).
However, researches have shown both CPM and brace do not play much role in decreasing the pain or increasing range the range of motion around patellofemoral joint (joint between the knee cap and condyles of the femur).
As a matter of fact, the rehabilitation of ACL depends upon the patient’s age, level of activity, and the future outlooks.
It also depends on the type of injury and the surgery performed.
Most of the times you may be recommended a home-based exercise program, which may consist of open – and closed- chain kinetic exercises, quadriceps-hamstring coactivation, strengthening of the calf muscles, leg balance exercises, plyometrics and stretching exercises.
Open-chain exercises after 6 weeks of surgery may improve the strength without affecting the graft.
As you continue to benefit from the program the goal changes from managing local damage to damage or defect in the other regions.
An immediate weight bearing after the surgery may decrease the pain in the patellofemoral joint.
Apart from regaining the strength of the affected extremity, it is also important to work on the normal extremity.

As ACL tear, may have long-lasting effects, a repetitive neuromuscular training should be encouraged to guarantee a long-term dynamic and stable knee.
Hydrotherapy, or aquatic training, is also useful to regain the strength of your quadriceps and hamstrings muscles.
If you want to reach your ACL knee rehabilitation goal or want to ask any questions regarding your ACL recovery, PCL or meniscus injury, contact Jazz Alessi now by clicking on this link, here.
References
Angoules AG, Balakatunis K, Boutsikari EC, Mastrokalos D, Papagelous PJ. Anterior-posterior instability of the knee following ACL reconstruction with bone-patellar tendon -bone ligament in comparison with four strands Hamstring autograft. Rehabil Res Pract, 2013;Jul.
Biggs A, Jenkins WL, Urch SE, Shelbourne KD. Rehabilitation of patients following ACL reconstruction: A knee symmetry model. N Am J Sports Phys Ther, 2009 Feb;4(1): 2-12.
Burkhart B, Ford KR, Myer GD, Heidt RS Jr, Hewett TE. Anterior cruciate ligament tear in an athlete: does increased heel loading Contribute to ACL repair? N Am J Sports Phys Ther, 2008 Aug;3 (3): 141-144.
Dambros C, Martimbianco ALC, Polachini LO. Effectiveness of cryotherapy after anterior cruciate ligament reconstruction. Acta Orthop Bras, 2012;20(5): 285-290.
Griffin L. The female athlete. In: Miller MD, Thopmson SR, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 4th ed. Philadelphia, PA: Elsevier Saunders; 2015:chap 32.
Hewett TE, Myer GD. The mechanistic connection between the trunk, knee, and anterior cruciate ligament injury. Exerc Sport Sci Rev, 2011 Oct;39(4): 161-166.
Kakarlapudi TK, Bickerstaff DR. Knee instability. West J Med, 2001 Apr;174(4): 266-272.
Malagelada F, Vega J, Golano P, Beynnon B, Ertem F.Knee anatomy and biomechanics of the knee In: Miller MD, Thopmson SR, eds.DeLee and Drez’s Orthopaedic Sports Medicine. 4th ed. Philadelphia, PA: Elsevier Saunders; 2015:chap 91.
Micheo W, Amy E, Sepulveda F. Anterior cruciate ligament tear. In: Frontera WR, Silver JK, Rizzo TD, eds. Essentials of Physical Medicine and Rehabilitation. 3rd ed. Philadelphia, PA: Elsevier Saunders; 2015:chap 63.
Ng WHA, Griffith JF, Hung EHY, et al. Imaging of the anterior cruciate ligament. World J Orthop, 2011 Aug;2(8): 75-84.
Niska JA, Petrigliano FA, McAllister DR. Anterior cruciate ligament injuries (including revision). In: Miller MD, Thopmson SR, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 4th ed. Philadelphia, PA: Elsevier Saunders; 2015:chap 98.
Noyes FR, Barber-Westin SD. Anterior cruciate ligament primary reconstruction: diagnosis, operative techniques, and clinical outcomes. In: Noyes FR, Barber-Westin SD, eds. Noyes’ Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes. 2nd ed. Philadelphia, PA: Elsevier Inc; 2017:chap 7.
Nyland J, Brand E, Fisher B. Update on rehabilitation following ACL reconstruction. Open Access J Sports Med, 201;1: 151-166.
Phillips BB. General principles of arthroscopy. In: Azar FM, Beaty JH, Canale ST, eds. Campbell’s Operative Orthopaedics. 13th ed. Philadelphia, PA: Elsevier Inc; 2017:chap 49.
Philips BB, Mihalko MJ. Arthroscopy of lower extremity. In: Azar FM, Beaty JH, Canale ST, eds. Campbell’s Orthopaedic Orthopaedics. 13th ed. Philadelphia, PA: Elsevier; 2017:chap 51.
Spindler KP, Wright RW. Anterior cruciate ligament (ACL) tear. N Engl J Med, 2008 Nov;359(20): 2135-2142.
Tselika-Garfe A, Effects of acute myocardial infarction on the patient’s and family’s way of life. Noseleutike, 1992 Jul-Sep;31(141): 190-200
Wright RW, Hass AK, Anderson J, et al. Anterior cruciate ligament reconstruction rehabilitation. Sports Heath, 2015 May;7(3): 239-243.
Disclaimer: This website and all its content is to be used for information purposes only. This website or any of its content or links to third parties does not diagnose, advise, treat or cure any ailments, illness or disease.
You agree to hold harmless the owner of this site for any action taken on your own without consulting your medical doctor first by using the information on the website for diagnostic, treatment, or any other related purposes. This is not medical advice. If you are suffering from any illness, disease or ailments please contact your doctor first and immediately.